A sponsor submits a dataset package to the FDA, and three weeks later the review team sends back a technical rejection. Not because the drug data was wrong. Because the SDTM domains and the ADaM datasets didn’t speak the same language the agency’s reviewers expected them to speak.
This happens more often than most clinical operations teams admit out loud. SDTM Programming Services and ADaM Dataset Programming are frequently treated as a single line item on a project plan – “CDISC deliverables” – when in reality they’re two distinct disciplines, built for two different audiences, governed by two different sets of rules.
If you’re preparing a regulatory submission, understanding where SDTM ends and ADaM begins isn’t academic. It’s the difference between a clean technical review and a Refuse-to-File letter that sets your timeline back months. This guide breaks down what separates the two standards, where teams most often get the relationship wrong, and what genuine CDISC Compliance Services actually look like in practice.
What SDTM Actually Is – And What It’s Not
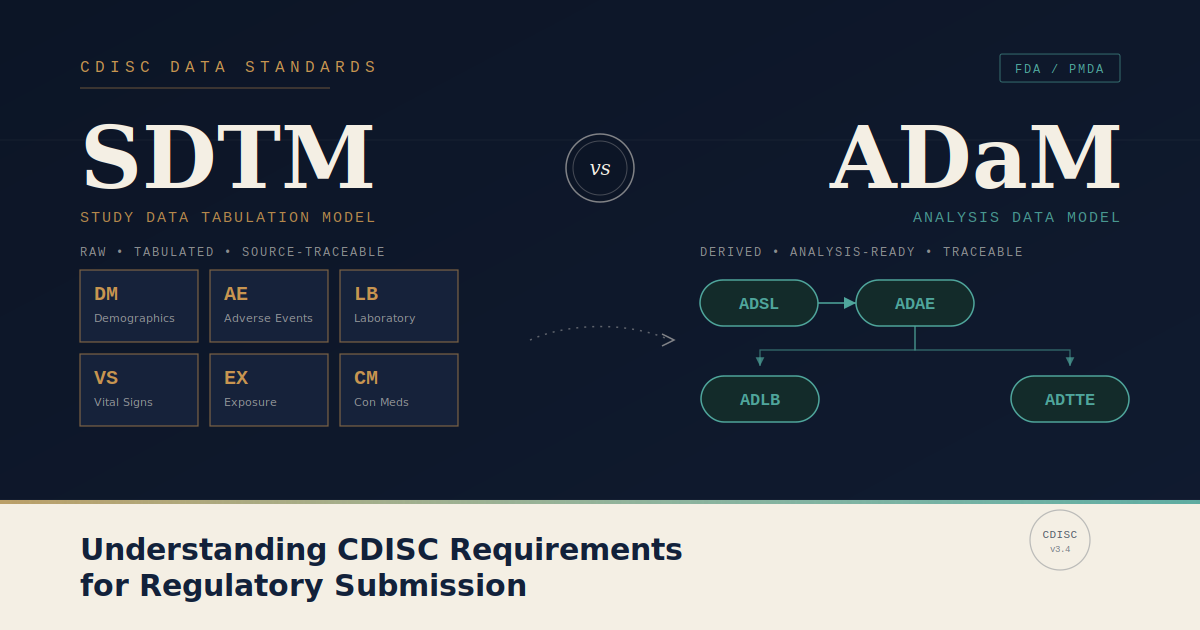
SDTM, the Study Data Tabulation Model, is CDISC’s standard for organizing raw clinical trial data into a consistent, submission-ready structure. It’s not analysis-ready. It was never meant to be.
Think of SDTM as the evidentiary record. Every domain – DM for demographics, AE for adverse events, LB for laboratory results – exists to represent what was collected, observed, or reported during the trial, traceable back to the source.
According to the FDA’s Study Data Technical Conformance Guide, SDTM datasets must demonstrate traceability to source data and adhere to controlled terminology published by the CDISC Controlled Terminology package in effect at study start. Reviewers are not just checking that the data exists – they’re checking that they can trace a single adverse event from the SDTM AE domain back to the case report form.
Key SDTM characteristics:
- Organized by domain (one observation class per dataset)
- One record generally represents one collected data point
- Variable names follow a fixed two-character domain prefix
- Built for traceability, not statistical analysis
- Validated against the SDTM Implementation Guide (SDTMIG) version specified in the study’s Define-XML
What ADaM Adds to the Picture
ADaM – Analysis Data Model – is where SDTM data gets transformed into something a statistician can actually run a model against. ADaM datasets are analysis-ready. They contain derived variables, flags, imputed values, and the population definitions that drive every table, listing, and figure in the clinical study report.
This is the layer where most of the actual statistical thinking happens.
An ADaM dataset doesn’t just restate what SDTM already shows. It answers a question: who’s in the efficacy population, what’s their last observation carried forward, which subjects were excluded and why. The CDISC ADaM Implementation Guide requires every analysis variable to be traceable back to its SDTM source, documented through the metadata in Define-XML, with no derivation left unexplained.
Key ADaM characteristics:
- Built for statistical analysis, not raw representation
- Includes derived and imputed variables (e.g., ADSL for subject-level analysis)
- Population flags (ITT, PP, Safety) live here, not in SDTM
- Every derivation must trace back to SDTM source variables
- Validated against the ADaM Implementation Guide (ADaMIG)
SDTM vs ADaM: A Side-by-Side Comparison
| Aspect | SDTM | ADaM |
|---|---|---|
| Purpose | Tabulate raw collected data | Support statistical analysis |
| Audience | Regulatory reviewers, data managers | Biostatisticians, medical writers |
| Structure | One domain per observation class | One dataset per analysis need |
| Record relationship | Mirrors source data collection | Derived, often one record per subject per analysis |
| Contains derived variables | Rarely | Extensively |
| Population definitions | Not applicable | Central (ITT, PP, Safety flags) |
| Traceability requirement | To source data (CRF) | To SDTM domains |
| Governing guide | SDTMIG | ADaMIG |
| Submission role | Evidentiary record | Analysis justification |
Why Sponsors Get the Sequence Wrong
The most common failure point isn’t poor programming. It’s sequencing.
Teams under deadline pressure sometimes start ADaM derivations before SDTM domains are finalized and locked. When an SDTM variable changes after ADaM programming has already begun, every downstream derivation has to be re-traced and re-validated. That rework can add two to four weeks to a submission timeline depending on the number of affected domains.
A second, quieter problem: inconsistent controlled terminology between SDTM and ADaM. If a SDTM domain uses one coding convention for a disposition variable and the ADaM layer derives a population flag from a slightly different version of that variable, the discrepancy often isn’t caught until validation – sometimes not until the agency’s own review.
The PHUSE CDISC Data Standards working groups have published repeated guidance on this exact failure mode, recommending that SDTM domains be frozen and validated before ADaM programming begins in earnest, not run in parallel as a time-saving shortcut.
What CDISC Compliance Actually Requires
Compliance isn’t a single validation report. It’s a chain of decisions made consistently from protocol design through final submission package.
A genuinely compliant submission package includes:
- SDTM domains validated against the current SDTMIG and controlled terminology version
- ADaM datasets with full traceability documented in Define-XML
- A Reviewer’s Guide for both SDTM (SDRG) and ADaM (ADRG) explaining study-specific decisions
- Pinnacle 21 (or equivalent) validation reports with all findings explained or resolved
- Consistent variable naming and controlled terminology across both layers
Two items, often overlooked:
- Define-XML version alignment with the SDTMIG/ADaMIG versions actually used
- Annotated CRFs cross-referenced against SDTM domain variables
The FDA’s Data Standards Catalog specifies which versions of SDTMIG and ADaMIG are acceptable for current submissions, and that catalog updates more frequently than most internal SOPs do. Submitting against a deprecated standard version is a documented cause of technical rejection, separate from any data quality issue.
Build vs Outsource: When to Bring In Specialized Programming Support
Some sponsors run SDTM and ADaM programming entirely in-house. Others bring in specialized support for one layer, or both, particularly for complex therapeutic areas or first-time submissions.
| Scenario | In-house may work | Outsourced support typically helps |
|---|---|---|
| Standard Phase II trial, established team | Yes | Optional |
| First FDA submission for the sponsor | Sometimes | Strongly recommended |
| Legacy data conversion to current CDISC standards | Rarely sufficient alone | Recommended |
| Multiple concurrent submissions | Resource-dependent | Often necessary |
| Complex oncology or rare disease endpoints | Case-by-case | Recommended |
The deciding factor usually isn’t team size. It’s whether the team has handled the specific SDTMIG/ADaMIG version combination, the specific therapeutic area’s domain quirks, and the specific agency’s recent review patterns – FDA and EMA conformance expectations are not identical, and a team fluent in one isn’t automatically fluent in the other.
Frequently Asked Questions
Q. What is the main difference between SDTM and ADaM?
SDTM organizes raw clinical trial data into standardized domains for regulatory review and traceability to source. ADaM transforms that SDTM data into analysis-ready datasets containing derived variables, population flags, and the structures statisticians need to generate tables, listings, and figures.
Q. Is SDTM required for all FDA submissions?
Yes. The FDA requires SDTM-formatted datasets for NDA, BLA, and ANDA submissions containing clinical study data, per the Study Data Technical Conformance Guide. Submissions that don’t conform to SDTM are subject to refusal-to-file or refusal-to-receive decisions.
Q. Can ADaM datasets be created without finalized SDTM domains?
Technically yes, but it’s not advisable. Building ADaM derivations against SDTM domains that are still being revised typically leads to rework once the source data locks, since every ADaM variable must trace back to a validated SDTM source.
Q. What is Define-XML and how does it relate to SDTM and ADaM?
Define-XML is the machine-readable metadata file that documents the structure, content, and origin of variables in both SDTM and ADaM datasets. It’s required for FDA and PMDA submissions and serves as the map reviewers use to understand dataset structure and derivations.
Q. Do EMA submissions have the same CDISC requirements as FDA?
EMA has moved toward CDISC standards but applies them with some differing expectations, particularly around dataset scope and reviewer guide content. Sponsors submitting to both agencies should confirm current requirements against each agency’s published technical conformance guidance rather than assuming parity.
Q. How long does CDISC-compliant SDTM and ADaM programming typically take?
Timelines vary by study complexity, but a mid-sized Phase II/III trial typically requires several weeks for SDTM domain creation and validation, followed by additional weeks for ADaM derivation and validation, run sequentially rather than in parallel for best results.
Conclusion
SDTM and ADaM aren’t two versions of the same task. One builds the evidentiary record; the other builds the analytical case. Submission packages fail not because sponsors lack CDISC knowledge in the abstract, but because the sequence, traceability, and version alignment between the two layers break down somewhere between protocol design and final package assembly. Get that sequence right, and the technical review becomes what it’s supposed to be – a confirmation of work already done correctly, not a discovery process.
Leave A Comment